This is my first one of these posts, so I’m going to backtrack a bit before circling back to the news I got last week.
BEFORE LAST WEEK
Breast Cancer
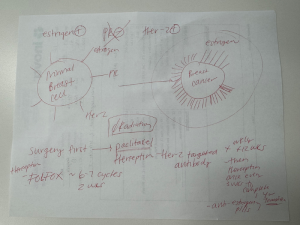
Once we learned that the third area of suspicion in my left breast was cancer—specifically invasive ductal carcinoma (IDC) with a HER2+ biomarker—I decided a mastectomy was the right answer.
At that point, they would have had to remove too much tissue to make a lumpectomy viable, and there was concern that the third tumor may have shed cells into my breast, or possibly even into my lymph nodes. So… left boob had to go.
During the mastectomy, they also performed a sentinel lymph node biopsy. A blue dye is injected during surgery and the lymph nodes that absorb it are tracked. The first node that turns blue is the one most likely to show spread, so it’s removed and tested. Additional nodes are taken until they no longer light up blue.
Going into surgery, we didn’t know the full extent of the IDC or whether there was lymph node involvement, which meant staging and treatment were still uncertain. Both chemotherapy and a five-year course of estrogen-blocking medication were on the table. Because I’m pre-menopausal, that medication would be Tamoxifen (post-menopausal women take a different one). Radiation was unlikely, since there would be no breast tissue left to radiate. Small wins?
Rectal Cancer
Rectal cancer works almost in the opposite way. They were able to stage it and lay out a treatment plan before surgery.
Originally, because of the high stage and my age, I was told I’d need the full neoadjuvant treatment path: chemotherapy, then radiation, then surgery.
I met with two oncologists and chose the second—largely because he works in the same cancer center as my breast team (his office is literally downstairs from theirs). He told me about a recent clinical trial showing that recurrence and survival rates were the same for patients who did chemo → surgery as for those who did chemo → radiation → surgery.
The catch: the tumor has to shrink enough for surgery to be feasible and safe.
So we’re going with a chemo-to-surgery plan and crossing our fingers that chemo gets me there—allowing me to skip radiation. Radiation—especially for rectal cancer—can have some pretty gnarly long-term side effects, and both my oncologist and the radiation oncologist were very clear that they want to avoid it if possible—especially given my age (and the fact that I’m single). I love that my team is focused not just on survivability, but on quality of life after treatment—when I won’t just be surviving, but thriving.
This is very much a one-step-at-a-time plan (though, honestly, they all are). I get my port placed on March 5, and we’ll start chemo—six to seven rounds of FOLFOX—on March 10.
UPDATE: WEEK OF FEBRUARY 23, 2026
There’s no update yet on the rectal cancer front. Just moving forward as planned!
Breast Cancer Update
During my mastectomy, my breast surgeon removed three lymph nodes, which is a relatively small number. My margins came back clear and there was no nodal involvement—HUGELY good news. I landed at Stage One breast cancer.
That said, this doesn’t mean rogue cancer cells couldn’t have escaped my breast and be floating around looking for another place to land. That risk is higher because of my HER2+ biomarker. (For those who like details: my DCIS was ER+/PR+ HER2-, and my IDC is ER+/PR- HER2+.) So, even with clear margins and nodes, I still need a full course of systemic treatment—exactly what we had anticipated going in.
I met my breast oncologist on Tuesday and she is fantastic. She walked into the room already having spoken with my rectal oncologist, fully aware of their plan, and told me she had taken my case to her tumor board (the third tumor board I’ve now been presented at). I love how my doctors talk to each other about me and my treatment before they even meet me. I feel incredibly well cared for. As a lifelong overachiever, I also feel a little fancy and a little famous. (Look, I’ll take any good feeling I can get.)
Because my rectal cancer is at a higher stage, it has to take priority. A full course of chemo (FOLFOX in this case) is non-negotiable. That means my breast cancer treatment has to be modified—and the two treatments have to happen at the same time. I thought I might do them back-to-back but evidently I can’t wait until the rectal cancer treatment is over, because any rogue breast cancer cells could have time to grow. So yes: I’ll be doing two chemos concurrently.
One thing I’ve learned is that each “chemo” is really a cocktail of medications. The standard breast cancer chemo regimen I would have done has two main components–paclitaxel and herceptin. I can’t have Paclitaxel because it would be too toxic to combine with FOLFOX. The good news is that two of the drugs in FOLFOX have been used to treat breast cancer in the past, and the entire breast tumor board is confident that, in my case, the FOLFOX drugs will be sufficient in place of Paclitaxel.
The unbelievably good news for me personally is that it’s Paclitaxel that makes you lose your hair. Of all the horrible news I’ve received in the last two months, not one piece has made me cry (in front of anyone). When my breast oncologist told me I would not lose my hair as a result of breast cancer treatment, I teared up and could hardly make words. I told her I was always afraid of getting breast cancer because a) it’s cancer and b) my boobs and my hair are two of my most favorite features, hands down. Anyway. Let’s go, small wins!
They will be adding Herceptin, which specifically targets HER2+ cancer cells. Each time I go in for my FOLFOX infusion I’ll get Herceptin first. The whole infusion process should take roughly five-hour hours. In a delightful plot twist, this apparently qualifies me for a private infusion room. Baller.
Even better, since my whole team works in the same building, my breast oncologist and dietitian have scheduled visits with me during infusion weeks and will come see me in my private room/office. Extremely fancy. Very boss-like. Which I am. Obviously.
I’ll do this Herception/FOLFOX infusion pattern every two weeks for six or seven rounds, starting March 10. After infusion day, I’ll be sent home with a chemo pump for 46 hours before returning to get unplugged and have my line flushed. Once I complete the six to seven rounds of FOLFOX, I’ll continue Herceptin every three weeks to complete a full year of treatment.
After surgery is finished (I will have two more that I’m aware of–a breast tissue expander-to-implant swap, and a rectal tumor removal), I’ll start Tamoxifen. I can’t take it before surgery because it increases the risk of blood clots, and we definitely don’t want that.
So that’s how all these seemingly disparate puzzle pieces are coming together—to treat two completely separate cancers at the same time.
More updates to come as things evolve, one step at a time.
1 Comment
Baller. Boss. Babe.